Navigation
- What is Station and Why Does It Matter?
- The Fetal Ejection Reflex, Ferguson Reflex and Medicated Births
- Why Laboring Down Can Make A Difference
- Key Take Aways
- Helpful Resources
Watch most movies or TV shows that show a hospital setting where a woman is giving birth and comments like “how dilated is she?” or “Oh, you are 10 cm, let’s start pushing!” are being thrown around. So it is no wonder that many people associate labor progress with one determining factor- cervical dilation. However, there is another key element to help decide when to start the actual birthing of the baby- station!
What Is Station and Why Does It Matter?
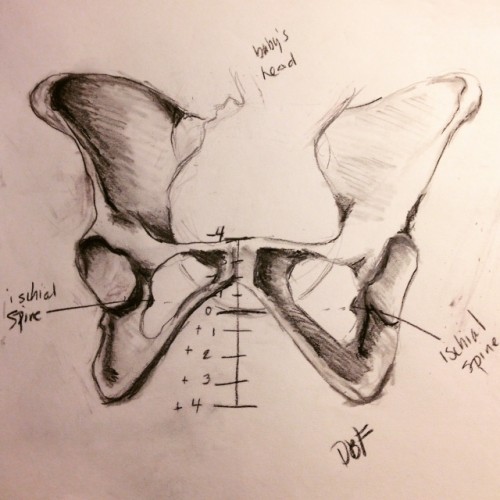
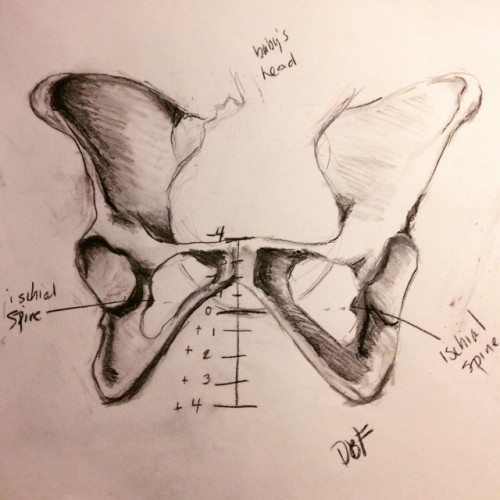
Station refers to the baby’s position in relation to the ischial spines of the birthing person’s pelvis. The ischial spines are small bony protrusions that can be felt during a vaginal exam to assess the baby’s descent. (Please resist the urge to check this yourself!)
- If the baby’s head has not yet descended into the pelvis, it is measured in negative numbers from -4 to -1.
- Once the head is aligned with the ischial spines, it is at 0 station.
- As the baby moves further down, it is measured in positive numbers from +1 to +4, with +4 indicating crowning.
Understanding the baby’s station can help determine the best time to start pushing, rather than relying solely on dilation.
The Fetal Ejection Reflex, Ferguson Reflex and Medicated Births
Some people experience an uncontrollable urge to push—one friend described it as “vomiting out of her vagina”. This powerful, involuntary physiological response is known as fetal ejection reflex coined by French obstetrician Michel Odent.
The Ferguson reflex and the fetal ejection reflex are related but distinct physiological responses during labor:
- Ferguson reflex: This is a neuroendocrine reflex triggered when the baby’s head presses on the cervix and vaginal walls, stimulating stretch receptors. This pressure signals the release of oxytocin, which increases the strength and frequency of contractions. It’s part of the feedback loop that helps labor progress.
- Fetal ejection reflex: this is a more intense, involuntary expulsion of the baby, often seen in undisturbed, unmedicated births. It’s characterized by powerful, uncontrollable pushing efforts—often described as the body taking over. It’s less about hormonal feedback and more about a sudden, instinctive action to birth the baby.
In short, the Ferguson reflex supports ongoing labor, while the fetal ejection reflex is a dramatic, often final push to get the baby out.
When someone has an epidural, both the Ferguson reflex and fetal ejection reflex can be significantly dampened or even completely inhibited due to the numbing effect on the lower body and pelvic nerves.
Why Laboring Down Can Make a Difference
In many hospital settings, once a mother starts pushing, she’s on the clock. Hospitals often have a time limit on pushing before interventions such as a C-section are recommended for reasons like “failure to progress.”
To help avoid unnecessary interventions, laboring down can be beneficial. This means allowing the uterus to continue contracting and moving the baby down passively before actively pushing. Since the mother isn’t feeling the full sensation of contractions in a medicated birth, waiting until the baby has reached a lower station before pushing can:
- Conserve energy—no unnecessary early pushing.
- Reduce time limits imposed by hospital policies.
- Increase the chances of a vaginal birth by allowing the body to do the work naturally before engaging in active pushing.
Key Takeaways
- Dilation is only part of the labor progress equation—station is equally important.
- The Ferguson reflex triggers an involuntary urge to push, but medicated births may not experience this.
- Laboring down can prevent exhaustion and reduce the likelihood of interventions like a C-section.
By understanding station, you can make informed decisions about when to push, saving energy and possibly avoiding unnecessary medical interventions. Knowledge is power! Happy birthing!
To learn more about the Prenatal Yoga Center and the classes that we offer. Click below to view our class schedule.
Helpful resources!
Podcast: JAMA (The Journal of the American Medical Association) Laboring Down Study; Yay or Nay?
Podcast: All Things Cervix!
What is the difference between a walking epidural and standard epidural?
Source
http://pregnancy.about.com/cs/laborbasics/a/pushing.htm
Drawing credit- ME! (deb flashenberg)