Sometimes walking into a hospital leaves you feeling like you just landed without warning in a foreign country. So many names and terms used today in hospitals may be unfamiliar to you! Rest assured, this quick glance glossary can help demystify labor and delivery talk and get you fluent in “labor lingo.”
Amniotomy- The artificial rupturing of the amniotic sac. This is done by the care provider with an amniotic hook, which looks like a crochet needle.
APGAR- A quick assessment of the newborn baby. Named after Virginia Apgar. The test is taken at 1 min after birth and then again at 5 min. The care provider is measuring Activity (muscle tone), Pulse (heart rate), Grimace (reflexes), Appearance (skin coloration), and Respiration (breathing rate and effort). These evaluations can all be done with the baby still on the mother’s chest or stomach.
Back Labor- Occurs when the baby’s back is against mother’s back. This leads to longer labors and more pain, especially in the mom’s lower back.
Dilation- The measurement of the opening of the cervix. This is measured in centimeters from 0-10, with zero being completely shut and 10 cm being fully open, thereby completing the first stage of labor. Dilation occurs as the baby’s presenting part presses down onto the cervix as the uterus is contracting and pulling the cervix upwards. It is not unusual for some women to have cervical dilation before the onset of labor.
Effacement- The softening and thinning of the cervix. This is measured on a % scale. 0% means the cervix is still long and hard, 100% means that cervix is completed thinned out. The 100% effacement is often referred to as a “paper thin” cervix.
Episiotomy- The cutting of the perineum (the space between the anus and the vagina) in order to make the vaginal opening larger.
*Side note: There is no evidence that an episiotomy reduces the risk of perineal injury, improves perineal healing, prevents birth injury in babies, or reduces the risk of future incontinence (involuntary loss of urine or feces). In fact, an episiotomy is associated with more pain, sexual problems, and incontinence after birth. Also, there is evidence that episiotomies done to prevent tears that the provider thinks are about to happen actually cause more tears (1).
External Fetal Monitor (EFM)- An external device used to listen to the heart rate of the baby. It is rather non evasive, but does limit the mother’s mobility.
*It should also be noted:
-Routine continuous EFM provides no benefit for babies and increases the risk of cesarean for mothers.
-The American College of Obstetricians and Gynecologists (ACOG) recommends that for healthy, low-risk women (almost all women), fetal heart rate be monitored with a fetoscope or Doppler every 30 minutes in active labor and every 15 minutes during pushing.
-The World Heath Organization (WHO) encourages intermittent manual listening and warns that EFM is often used inappropriately (2).
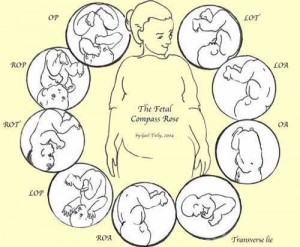
Fetal Position- The position in which the baby is situated in the pelvis.
-Head down is called vertex.
-Head up is called breech.
-Head down with the baby’s spine facing towards mother’s belly is called Anterior
– Occiput Anterior (OA)
-Right Occiput Anterior (ROA)
-Left Occiput Anterior (LOA)
-Head down with the baby’s spine facing mother’s back is call Posterior
– Occiput Posterior (OP)
– Right Occiput Posterior (ROP)
-Left Occiput Posterior (LOP)
 (Photo 2)
(Photo 2)Internal Fetal Monitor (IFM)- The internal monitor is used if the mother is high risk or the care provider does not feel like he/she is getting an accurate read from the external monitor. This monitor is more invasive since the amniotic sac has to be ruptured in order to use it. A small fetal scalp electrode is placed in the baby’s scalp to pick up the heart rate.
Meconium- Baby’s first stool. It is blackish, greenish and thick like tar. If the baby passes this stool during labor, the amniotic fluid will be tainted a darkish color. This is recognized as a sign of fetal distress.
Pitocin- The synthetic form of oxytocin. This is used in inductions and if the care providers feels the uterus needs a little help in contracting.
“Ring of Fire”- A burning or stretching sensation experienced as the baby is crowning and the head stretches out the perineum.
Station- The measurement of the baby’s decent through the pelvis. This is done by determining the baby’s presenting part (usually the head) in relation to the mother’s ischial spine. The highest point is -4, 0 would be when the head is in line with the ischial spine and at +4 the baby is on the perineum.
 (Photo 3)
(Photo 3)Transition- The final part of the first stage of labor as the mother is dilating from 8-10cm. This is the quickest stage and often the most intense with contractions 1 to 3 minutes apart.
Triage- Before you get admitted into the Labor and Delivery Unit, you will stop in “triage” to get checked out. There they will check your dilation and then listen to your baby for about 20 minutes with the external fetal monitors. Your doctor may or may not be there at this time. If your doctor is not in the hospital, a resident or possibly an attendant will perform the exam before notifying your doctor of your status.
Sources
1. “Care Practice Papers” from the Lamaze Institute for Normal Birth.
2. Lamaze International, teaching handout
Photo 2 Doula Momma
Photo 3 Blessed Mom




